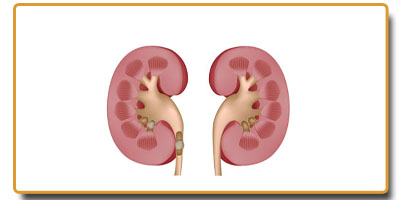
 Urinary stones could be found in the kidneys or in the ureters (tube that connects the kidney and the bladder). This is formed by precipitation of salts in the urine. Most commonly stones form from calcium, but they can also form from a variety of other materials including uric acid from gout. To note is that these stones are different from the stones formed in the urinary bladder which , inevitably is related to bladder outflow obstruction and urinary stasis.
Urinary stones could be found in the kidneys or in the ureters (tube that connects the kidney and the bladder). This is formed by precipitation of salts in the urine. Most commonly stones form from calcium, but they can also form from a variety of other materials including uric acid from gout. To note is that these stones are different from the stones formed in the urinary bladder which , inevitably is related to bladder outflow obstruction and urinary stasis.
Most small stones will pass spontaneously with hydration. Though the process is painful , it is accomplished with or without the help of a medication called Tamsulosin.
However stones more than 4 mm and especially more than 6 mm may not come out and hence will require other modalities of treatment. When stones are too large to pass, surgery is indicated to remove them. A ureteral stent may be required to relive blockage, or infection. A ureteral stent is a plastic tube placed between the kidney and the bladder with curly pigtails keeping them in place. In addition t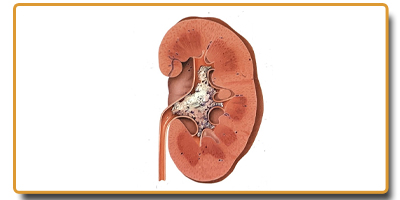 o reliving the blockage, it allows the ureter to dilate for a subsequent ureteroscopy.
o reliving the blockage, it allows the ureter to dilate for a subsequent ureteroscopy.
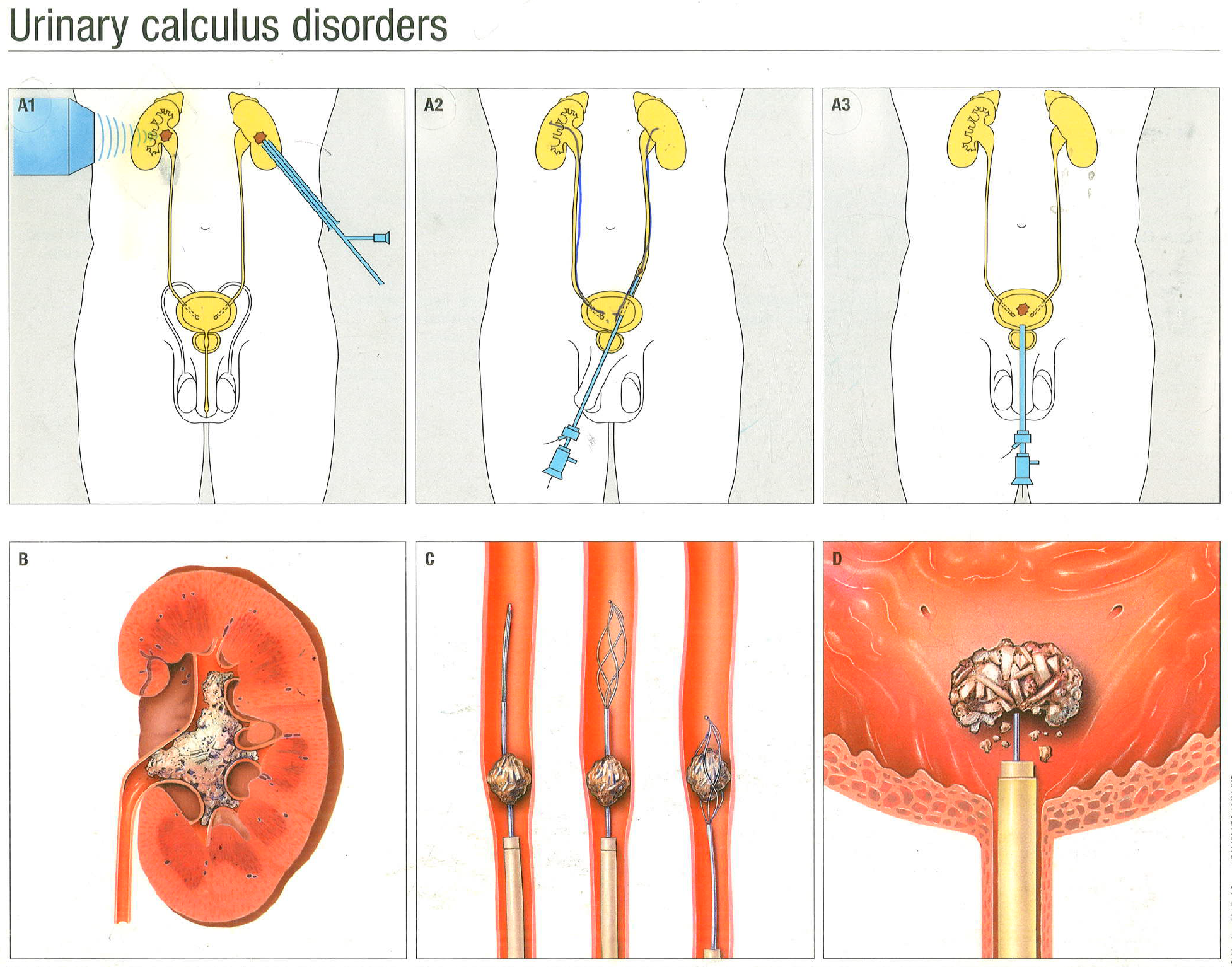
Ureteric stones could be treated with ureteroscopy ( tiny camera passed through the urine pipe and into the ureter) and lithotripsy (breaking of stones which could be achieved by either LASER or lithoclast). In addition, these stones can also be treated with ESWL (External shock wave lithotripsy). This is a non-invasive technique of breaking the stones by targeting shockwaves on the stones using X ray guidance. Done over 30 min, this procedure minimally painful and will require sedation. Patients are expected to have blood in their urine and some soreness in the side where the lithotripter has touched the skin. Rare complications include bleeding around the kidney. This procedure would be appropriate for stones that are in the kidney or high in the ureter.
 Ureteroscopy and laser lithotripsy:
Ureteroscopy and laser lithotripsy:
A small scope is passed through the urethra into the bladder and up the ureter to the stone. The stone can be visualized directly and is broken up using a small laser fiber or Lithoclast. Stone fragments will be broken to dust or removed with a basket. Patients are most often left with a temporary plastic stent that is internal and is removed after few weeks (4-6) with a flexible cystoscope.
Percutaneous nephrolithotomy (PCNL):
This is especially useful for stones more than 1 cm in the kidneys as this technique has the best stone clearance rates. A hole to the kidney is made from the back for introducing a telescope. Subsequently the stone is broken with lithoclast and the fragments are then removed. A drain is placed which is removed after a day or two.
Reduction of stone recurrence
Patients who had urinary stones have a good chance of it coming back in future. Measures could be adopted to reduce the chance of recurrence. 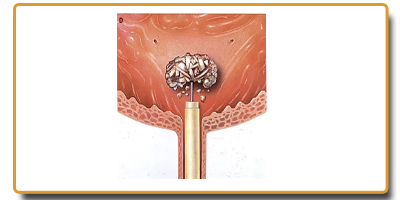 Hydration with about 3 litres of water (for an average adult) is the best method to reduce the chances of stones in future. Patients who had stones need a few blood tests as well as urine test which will be organised by the doctor.Minimising the salt, meat, chocolate, spinach, and cabbages would be a good idea. Fizzy drinks are best avoided. Appropriate calcium levels are essential and hence calcium restriction is no longer recommended.
Hydration with about 3 litres of water (for an average adult) is the best method to reduce the chances of stones in future. Patients who had stones need a few blood tests as well as urine test which will be organised by the doctor.Minimising the salt, meat, chocolate, spinach, and cabbages would be a good idea. Fizzy drinks are best avoided. Appropriate calcium levels are essential and hence calcium restriction is no longer recommended.